At Kalra Brain & Spine, when we counsel patients before an anterior cervical discectomy and fusion (ACDF), Dr. Kalra’s goal is not simply to explain the operation, it is to ensure that his patients understand the diagnosis, alternatives, expected benefits, risks, recovery, and long-term implications. We believe in, helping our patients develop realistic expectations regarding the outcomes of their cervical spine surgery. At Kalra Brain & Spine, we strive to ensure our patients are educated, informed, and share in the decision making process regarding their cervical spine surgery.
Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed operations for cervical radiculopathy (pinched nerves), cervical myelopathy (spinal cord compression), and degenerative disc disease. For appropriately selected patients, it can provide substantial improvement in arm pain, neurological symptoms, function, and quality of life. However, no surgery is right for every patient, and every operation carries risks.
Being prepared with the appropriate questions to ask your surgeon will allow you to make an informed decision regarding your condition and potential cervical spine surgery. Before proceeding with surgery, consider asking your surgeon questions from this recommended list.
Q: What Exactly Is The Problem You Are Treating?
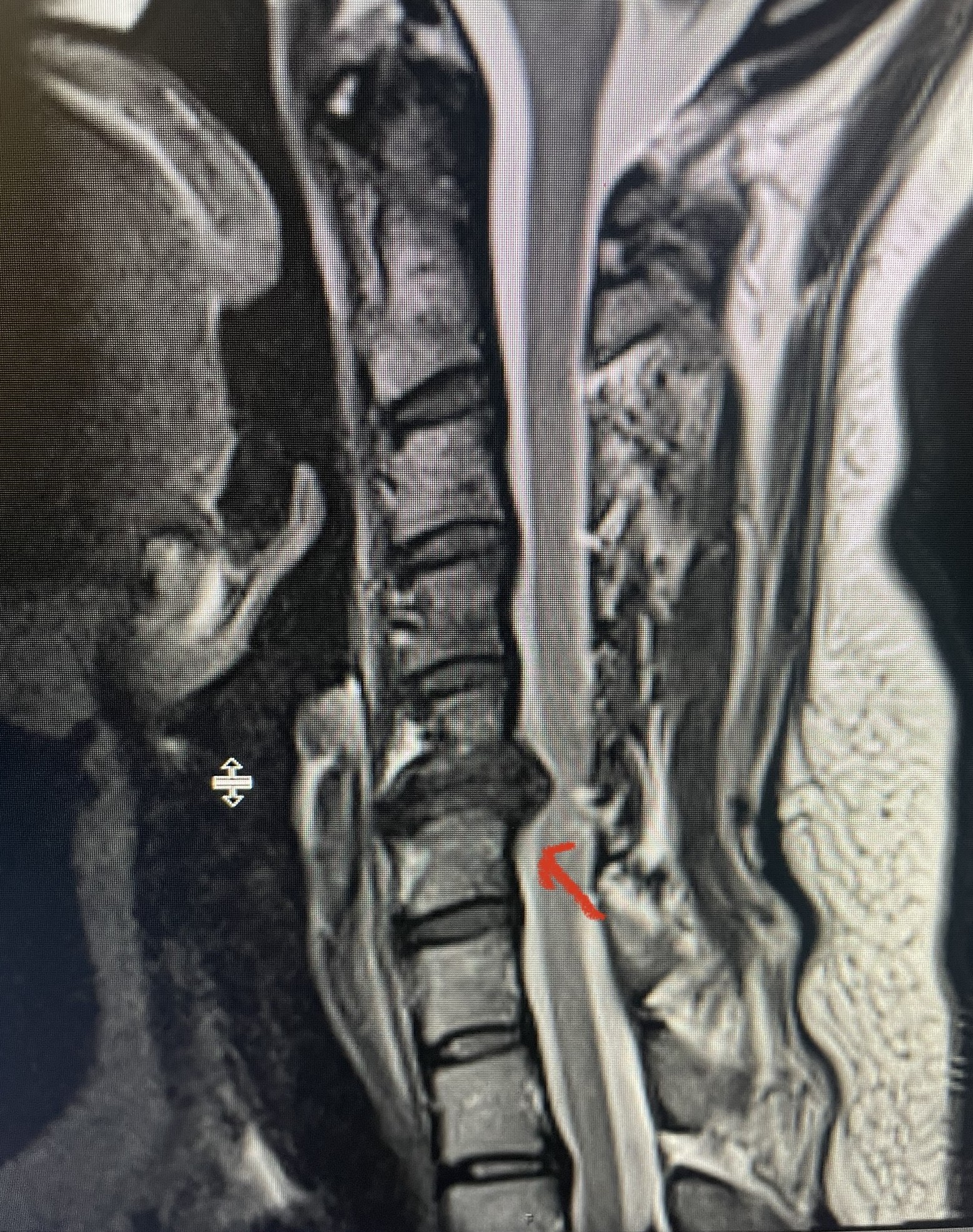
Ask your surgeon to show you the MRI or CT scan and explain:
- Which level(s) are abnormal?
- Is the spinal cord compressed?
- Is a nerve root compressed?
- What symptoms are coming from those findings?
- Which symptoms may not improve after surgery?
Patients often assume all neck, shoulder, arm, headache, and balance symptoms arise from the cervical spine. In reality, some symptoms may have other causes. Your surgeon should be able to explain precisely how your imaging findings correlate with your symptoms.
Q: Why Do You Recommend ACDF For Me?
Ask:
- Why is ACDF the preferred operation?
- Why not continue non-operative treatment?
- Why not perform a posterior decompression?
The best surgical procedure depends on the diagnosis, spinal alignment, number of levels involved, instability, bone quality, age, and other factors. Your surgical plan should be individualized rather than based on a one-size-fits-all approach.
Q: Is Cervical Disc Replacement An Option For Me?
Ask:
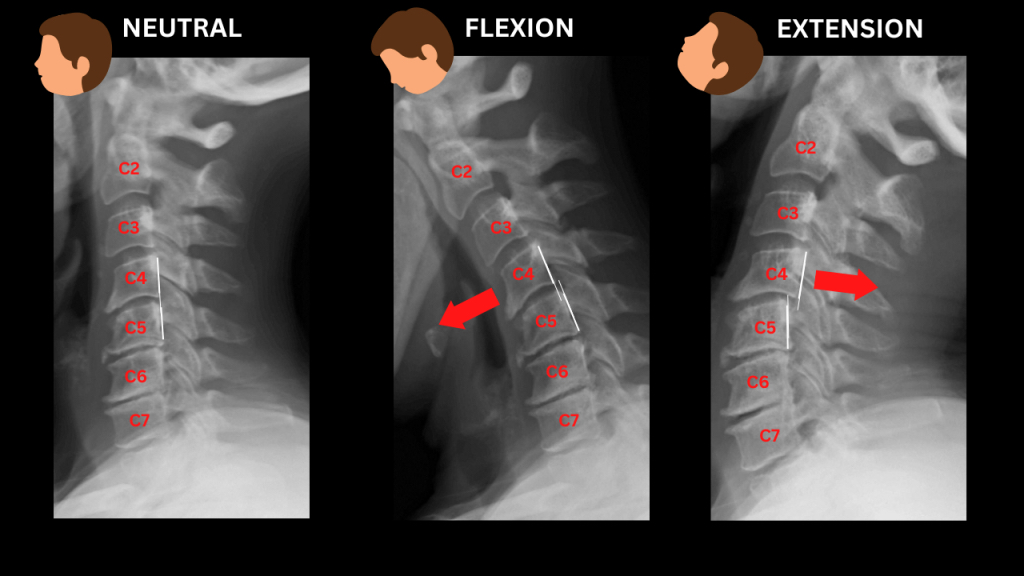
- Do I have structural spinal instability?
- Do I have severe arthritis or bone spurs in my facet joints?
- Will I have a better range of motion versus an ACDF?
- Does the recovery time differ with a cervical disc versus ACDF?
- Will I achieve the same symptom relief and outcome with cervical disc replacement?
- What are the advantages, and potential disadvantages of cervical disc replacement?
- How many cervical disc replacements do you perform in a year?
If you have structural instability and/or severe arthritis or bone spurs in your facet joints an ACDF will be the more appropriate surgical recommendation. Although cervical disc replacement does provide benefits such as a shorter recovery, better range of motion, and reduced risk for future surgery due to adjacent segment disease you most likely will not be a candidate with these conditions. Also, if your cervical spine surgery has been recommended for more than two levels (i.e. C4-7) you will most likely not be a candidate for cervical disc replacement as it is only indicated for one or two levels.
Q: What Happens If I Do Not Have Surgery?
This is one of the most important questions.
Ask:
- Is surgery elective or urgent?
- What is the risk of permanent nerve damage?
- Could spinal cord compression worsen?
- Can I safely continue conservative treatment?
For some patients with severe cervical myelopathy, delaying surgery may increase the risk of irreversible neurological decline. For others with stable radiculopathy, additional non-operative treatment may be reasonable.
Q: What Are The Chances That My Symptoms Will Improve?
Ask for expectations regarding the specific symptoms you are experiencing.
- Arm pain
- Numbness
- Weakness
- Neck pain
- Balance problems
- Hand dexterity
- Ability to return to work
Studies on ACDF patients consistently show meaningful improvement in pain and function for most patients, but outcomes vary by diagnosis, duration of symptoms, and neurological status before surgery. Some symptoms improve rapidly, whereas weakness or numbness may recover slowly or incompletely.
Q: What Symptoms Are Unlikely To Improve?
Many patients ask what surgery can accomplish but forget to ask what it may not.
Ask:
- Which symptoms are most likely to remain?
- Is any nerve damage permanent?
- How much neck pain is mechanical versus nerve-related?
A thoughtful surgeon should discuss both expected improvements and limitations.
Q: How Many ACDF Procedures Do You Perform Each Year?
Evidence suggests that surgeon experience and procedural volume are associated with lower complication rates in anterior cervical spine surgery. Higher-volume surgeons and surgical centers generally report fewer adverse events and better outcomes.
Ask:
- How many ACDFs do you perform annually?
- Is this operation routine in your practice?
- Does the surgical facility regularly do spine cases, specifically ACDFs?
Q. What Are The Specific Risks In My Case?
Every patient should understand both common and uncommon complications.
Ask your surgeon to discuss:
- Difficulty swallowing (dysphagia)
- Hoarseness or voice changes
- Infection
- Bleeding or hematoma
- Nerve injury
- Spinal cord injury
- Failure of fusion
- Hardware complications
- Need for future surgery
Dysphagia is among the most common complications following ACDF, although severity and duration vary considerably among patients. Multilevel procedures generally carry a higher risk than single-level procedures.
Q: What Is My Risk Of Not Achieving A Solid Fusion?
Fusion success is a major determinant of long-term outcomes.
Ask:
- What factors increase my risk of pseudarthrosis?
- Does smoking affect the fusion success?
- Does osteoporosis, diabetes, or other medical conditions increase risk?
- How will my fusion be monitored?
Pseudarthrosis rates vary depending on the number of levels fused, patient characteristics, and surgical technique.
Q: Will I Lose Motion In My Neck?
A fusion intentionally eliminates movement at the treated level.
Ask:
- How much neck motion will I lose?
- Will I notice a difference in daily activities?
- Does the number of fused levels matter?
Most patients tolerate loss of motion well after a one-level fusion, but multilevel fusions may have a more noticeable effect on cervical mobility.
Q: What Is Adjacent Segment Disease, And What Is My Risk?
Adjacent segment disease (ASD) refers to degeneration occurring at levels next to a fusion that becomes clinically significant.
Ask:
- What is my long-term risk?
- Are there factors that increase my risk?
- Could I need another surgery in the future?
Recent systematic reviews have identified factors such as cervical alignment and developmental canal stenosis as contributors to ASD risk after ACDF.
Q: What Type Of Implant, Cage, Graft, Or Plate Will Be Used?
Ask:
- What implant do you use?
- Why do you prefer it?
- Will you use a plate?
- Will bone graft come from me, a donor, or a synthetic source?
As patients you do not need to become implant experts, but understanding the rationale behind the chosen construct helps you participate in decision-making.
Q: How Long Will Recovery Take?
Ask for a realistic timeline regarding:
- Hospital stay
- Driving
- Return to desk work
- Return to physical work
- Exercise
- Sports and recreation
Recovery timelines differ significantly between a healthy patient undergoing a single-level ACDF and someone with many comorbidites and/or risk factors undergoing a multilevel fusion.
Q: Will I Need A Cervical Collar?
Patterns vary by practice and surgeon.
Ask:
- Do you routinely prescribe a collar?
- For how long?
- What evidence supports its use in my case?
Understanding postoperative restrictions beforehand helps avoid potential surprises.
Q: What Restrictions Will I Have After Surgery?
Ask specifically about:
- Lifting limits
- Travel
- Work activities
- Exercise
- Physical therapy
The answer should be individualized to your procedure and occupation.
Q: What Warning Signs Should Prompt Me To Call You?
Every patient should leave the office knowing which symptoms require urgent evaluation.
Examples include:
- Difficulty breathing
- Progressive swallowing problems
- New weakness
- Increasing numbness
- Fever
- Wound drainage
- Severe neck swelling
Although serious complications are uncommon, early recognition is imperative.
Q: What Will Success Look Like One Year From Now?
This question often reveals more than any other.
Ask your surgeon:
- What outcome would you consider excellent?
- What outcome would be average?
- What outcome would be disappointing?
A surgeon who can define realistic expectations is helping you make an informed decision.
The Most Important Question
If you only ask one question before an ACDF, it should be:
“Given My MRI Findings, Symptoms, Age, Health Status, And Goals, Why Is Surgery The Best Option For Me Right Now?”
A high-quality answer should include the diagnosis, alternatives, expected benefits, risks, and consequences of doing nothing. If you understand those elements clearly, you are in a much stronger position to make an informed decision.
The best spine consultations are not those in which patients ask the fewest questions, they are those in which patients leave understanding exactly why surgery is being recommended, what it can realistically accomplish, and what risks they are accepting. This is the foundation of shared decision-making and informed consent.
Q: Why Kalra Brain & Spine?
Answer:
At Kalra Brain & Spine in Frisco, Texas, Ricky Kalra, M.D. is a board certified, spine fellowship trained neurosurgeon who specializes in conservative management, second opinions, and minimally invasive spine surgery for the treatment of spinal pathologies. Dr. Kalra is known for his bedside manner and has stated “One of the most important things we do at Kalra Brain & Spine is to make sure our patients have all the information they need about their condition and treatment options so they can make an informed decision about their health care.”Dr. Kalra has been recognized as a D Best Neurosurgeon in Dallas by his fellow colleagues from 2017-2025.
If you’re struggling with ongoing cervical spine issues, a consultation with a specialized spine practice like Kalra Brain and Spine can help clarify your diagnosis, explore your options, and determine whether surgery is appropriate. At Kalra Brain and Spine, the goal is not surgery, it’s education with long-term functional improvement and quality of life.
If you have unanswered questions about your cervical spine pathology or recommended surgery, contact Kalra Brain & Spine at (972) 905-9226 or request an appointment on our website.